ACRC researcher John Harley awarded University of Alaska coronavirus response grant
As the novel COVID-19 virus disrupts life across the nation and world, many companies, organizations, and individuals are pivoting from their work to aid in response efforts. Dr. John Harley, a postdoctoral researcher at ACRC, hopes to fill a critical information need for COVID-19 vulnerability in Alaska. Though his work using environmental data to predict harmful algal blooms is unrelated to the current public health crisis, Harley saw an opportunity to use his background managing and visualizing large datasets to provide a valuable resource for COVID-19 response planning.
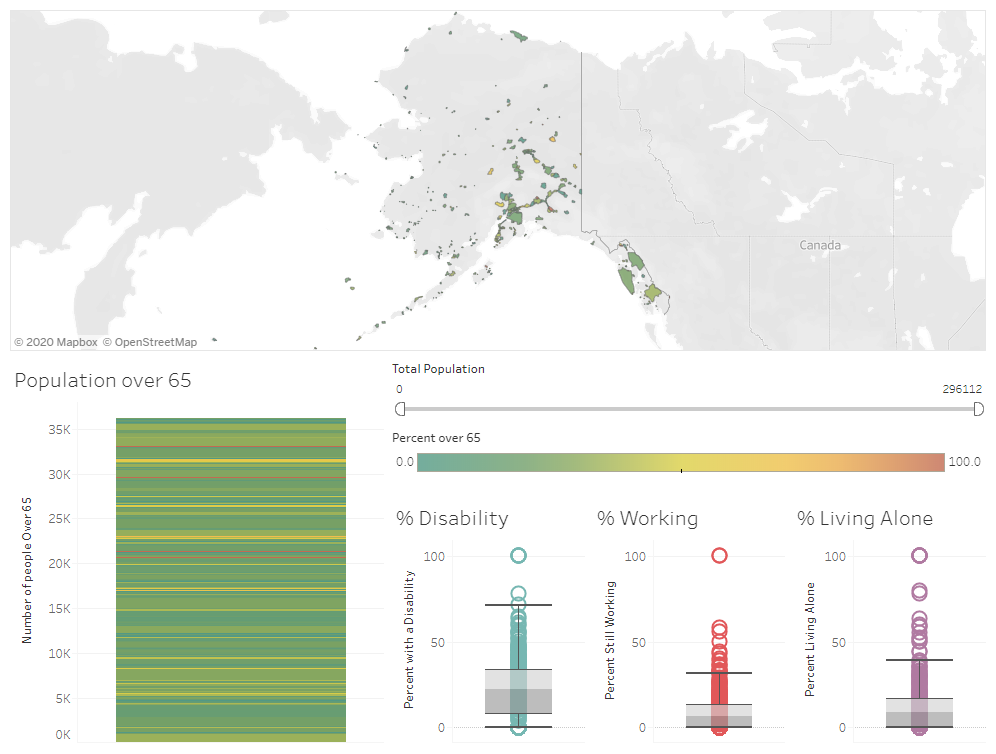
Harley was awarded $5,000 by the Immediate Innovation for Coronavirus Project (IICP) through the UAF Center for Innovation, Commercialization, and Entrepreneurship to create a tool providing a community-scale assessment of Alaska’s vulnerable populations. In the case of COVID-19, this includes those with pre-existing conditions (heart disease, compromised immune systems), smokers, and people 65 years and older. The recent call for proposals from the IICP sought to fund innovations that would improve the response and adaptation to COVID-19 immediately or in the longer term.
Local-scale vulnerability information is crucial for allocating resources and prioritizing high-risk areas during a pandemic. Currently, resources like the U.S. Centers for Disease Control and Prevention Social Vulnerability Index summarize social, demographic, and health data on a borough or census-area level. In most regions of the U.S., where census areas are often small and interconnected by roads, these tools are likely the most efficient way to map vulnerability. But census areas in Alaska can be as large or larger than entire states in the lower 48 and can contain dozens of isolated communities. “In northern Alaska, the Yukon Koyukuk census area is about the size of Montana, but people aren’t living everywhere in that census area. There are defined communities where people are living that might have different risk factors or demographics,” said Harley.
Determining community-level vulnerability for Alaska will aid health officials in making critical choices about the distribution of health care equipment and services.
Seeing the gap in vulnerability data at a scale relevant to Alaska communities, Harley proposed a solution. Using demographic information collected on a community (or census-designated place) level by the American Community Survey (ACS), Harley will examine risk factors and produce a tool for mapping community vulnerability to COVID-19. While Alaska is covered by only 29 census areas, the ACS designates 334 cities and census-designated places in the state.
“What I proposed is to look at those same risk factors and demographics, but on a smaller scale, so we can start to not only see where people are actually living within those census areas but also if there are differences between some of these communities in terms of their risk or vulnerability that might not be immediately apparent if you just look at the census area as a whole,” said Harley.
The resulting tool could assess risk factors relevant not only to COVID-19 response efforts but for any circumstance or event affecting vulnerable populations, including contagious diseases in the future. “You can tweak factors to particular diseases once you know the particular at-risk populations for a disease. It’s a fairly adaptable index that came be used for assessing risk for multiple diseases,” said Harley.